Fill in Your Rem Iowa Service Application Template
Fill in Your Rem Iowa Service Application Template
W-4 Example - To claim an exemption, employees must clearly write "EXEMPT" on the form and note the effective year.
To ensure a smooth application process for obtaining or renewing your nursing license, it is important to thoroughly understand the requirements set forth by the Arizona Board of Nursing. This form is not only vital for aspiring nursing professionals but also provides important information on advanced practice and program establishment. For those seeking clarity on the application details, click here to get the document to guide you through each necessary step and requirement.
Iowa Cremation Laws - Individuals may indicate if they waive the right to positive identification of the deceased.
Iowa Lead Safety - The seller must provide all known documentation related to lead hazards.
The Individualized Service Plan (ISP) is a document that shares similarities with the Rem Iowa Service Application form. Both documents are designed to assess an individual's needs and preferences regarding services. The ISP outlines specific goals and objectives tailored to the individual, ensuring that the services provided align with their unique circumstances. Like the Rem Iowa form, the ISP requires detailed personal information, including medical history and current living situations, to develop a comprehensive plan for care and support.
When dealing with the sale of a trailer, having a properly executed Trailer Bill of Sale form is essential to ensure a smooth transaction. This legal document not only records the sale and transfer of ownership but also provides a comprehensive record that details the terms of the sale, including the identities of both the buyer and seller. For those looking to formalize the sale process, it is highly recommended to visit https://billofsaleforvehicles.com/editable-trailer-bill-of-sale/ for a customizable template that suits individual needs.
The Application for Benefits is another document that parallels the Rem Iowa Service Application. This form is used to determine eligibility for various assistance programs. Both forms require personal details, financial information, and medical history to evaluate the applicant's needs. The Application for Benefits focuses on financial assistance, while the Rem Iowa form emphasizes service eligibility, but both aim to ensure that individuals receive the support they need.
The Medicaid Application is similar to the Rem Iowa Service Application in that it seeks to gather information to establish eligibility for services. Both documents require applicants to provide personal information, including income and medical conditions. The Medicaid Application specifically assesses financial eligibility for healthcare services, while the Rem Iowa form focuses on identifying the appropriate community services for individuals with developmental disabilities or mental health issues.
The Case Management Referral Form also shares commonalities with the Rem Iowa Service Application. This form is utilized to initiate the case management process, gathering essential information about the individual’s needs. Both documents require detailed personal data and history of services received. The Case Management Referral Form is more focused on connecting individuals to appropriate resources, while the Rem Iowa form is centered on applying for specific services.
The Health Assessment Form is another document that aligns with the Rem Iowa Service Application. Both forms collect comprehensive health information to evaluate the applicant’s needs. The Health Assessment Form typically includes questions about medical history, medications, and any disabilities. This information is crucial in determining the appropriate level of care and services, similar to the goals of the Rem Iowa application.
The Family Support Application is comparable to the Rem Iowa Service Application in that it seeks to understand the family dynamics and support systems of the individual. Both documents require information about family members, their roles, and any financial assistance received. The Family Support Application focuses more on the family’s ability to provide care, while the Rem Iowa form emphasizes the individual’s specific service needs.
Finally, the Service Coordination Plan bears resemblance to the Rem Iowa Service Application. This plan outlines the coordination of services for individuals with disabilities, ensuring that all aspects of care are addressed. Both documents require detailed information about the individual's needs, preferences, and current services. The Service Coordination Plan emphasizes the collaboration between various service providers, while the Rem Iowa form focuses on the application process for specific community services.
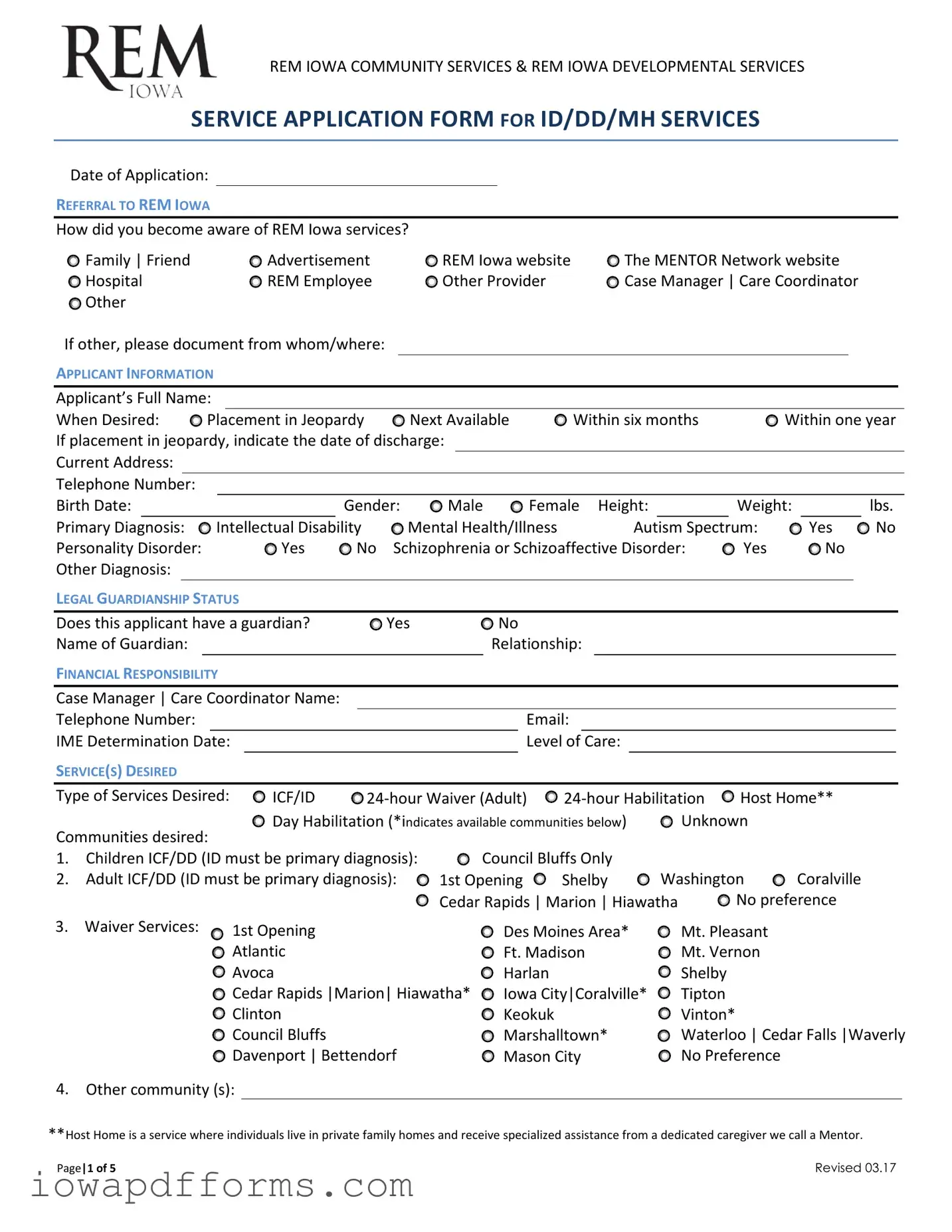
The REM Iowa Service Application form is an essential document for individuals seeking services related to intellectual disabilities, developmental disabilities, or mental health. Along with this form, several other documents may be required to support the application process. Each of these documents provides crucial information that helps assess eligibility and determine the appropriate services needed.
Gathering these documents ensures a comprehensive review of the application, allowing for the best possible support and services to be provided. Each document plays a vital role in understanding the applicant's unique needs and circumstances.
When filling out the Rem Iowa Service Application form, there are important guidelines to follow. Here’s a list of things to do and avoid:
REM IOWA COMMUNITY SERVICES & REM IOWA DEVELOPMENTAL SERVICES
SERVICE APPLICATION FORM FOR ID/DD/MH SERVICES
Date of Application:
REFERRAL TO REM IOWA
How did you become aware of REM Iowa services?
|
Family | Friend |
|
|
|
|
|
|
Advertisement |
|
|
REM Iowa website |
The MENTOR Network website |
|
|
|
|
|
|||||||||||||||||||||
|
Hospital |
|
|
|
|
|
|
REM Employee |
|
|
Other Provider |
|
|
Case Manager | Care Coordinator |
|
|
|
|
|
|||||||||||||||||||
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
If other, please document from whom/where: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
APPLICANT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Applicant’s Full Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
When Desired: |
|
|
|
Placement in Jeopardy |
|
Next Available |
Within six months |
|
Within one year |
|
||||||||||||||||||||||||||||
If placement in jeopardy, indicate the date of discharge: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
Current Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Telephone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Birth Date: |
|
|
|
|
|
|
|
|
|
Gender: |
Male |
|
Female |
Height: |
|
|
Weight: |
|
|
lbs. |
|
|||||||||||||||||
Primary Diagnosis: |
|
Intellectual Disability |
|
Mental Health/Illness |
|
|
|
Autism Spectrum: |
|
Yes |
No |
|||||||||||||||||||||||||||
Personality Disorder: |
|
|
|
|
|
|
Yes |
No |
Schizophrenia or Schizoaffective Disorder: |
Yes |
|
No |
|
|
|
|
|
|||||||||||||||||||||
Other Diagnosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
LEGAL GUARDIANSHIP STATUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Does this applicant have a guardian? |
|
|
Yes |
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Name of Guardian: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relationship: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
FINANCIAL RESPONSIBILITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Case Manager | Care Coordinator Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Telephone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
IME Determination Date: |
|
|
|
|
|
|
|
|
|
|
|
|
Level of |
Care: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
SERVICE(S) DESIRED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Type of Services Desired: |
|
|
ICF/ID |
|
Host Home** |
|
|
|
|
|
||||||||||||||||||||||||||||
Communities desired: |
|
|
Day Habilitation (*indicates available communities below) |
Unknown |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
1. Children ICF/DD (ID must be primary diagnosis): |
|
Council Bluffs Only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
2. |
Adult ICF/DD (ID must be primary diagnosis): |
1st Opening |
Shelby |
Washington |
Coralville |
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cedar Rapids | Marion | Hiawatha |
No preference |
|
|
|
|
|
|||||||||||||||
3. |
Waiver Services: |
|
|
|
|
1st Opening |
|
|
|
|
|
|
|
Des Moines Area* |
Mt. Pleasant |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
Atlantic |
|
|
|
|
|
|
|
Ft. Madison |
|
|
Mt. Vernon |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
Avoca |
|
|
|
|
|
|
|
Harlan |
|
|
|
|
Shelby |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
Cedar Rapids |Marion| Hiawatha* |
Iowa City|Coralville* |
Tipton |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
Clinton |
|
|
|
|
|
|
|
Keokuk |
|
|
|
|
Vinton* |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
Council Bluffs |
|
|
|
|
|
|
|
Marshalltown* |
Waterloo | Cedar Falls |Waverly |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
Davenport | Bettendorf |
|
|
|
Mason City |
|
|
No Preference |
|
|
|
|
|
|
|
|
|
|
||||||||||||
4. |
Other community (s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
**Host Home is a service where individuals live in private family homes and receive specialized assistance from a dedicated caregiver we call a Mentor.
Page|1 of 5 |
Revised 03.17 |

HISTORY OF SERVICES
Residential/
Has the applicant always lived at home? |
Yes |
No |
|
|
|
|
|
Service |
|
Provider |
|
|
|
|
|
Dates
Day/Vocational Services |
|
|
|
|
|
Has the applicant ever been employed: |
Yes |
No |
At a day program? |
Yes |
No |
Service
Provider
Dates
REFERRAL HISTORY
Has the applicant ever been arrested? |
Yes |
No |
If yes, provide: Date(s):
Reason(s):
Outcomes:
Does the applicant have a current court committal? |
Yes |
No |
|
|
||
Has the applicant been accused/convicted of sexual abuse? |
|
Yes |
No |
|||
If yes, provide: Date(s): |
|
|
|
|
||
Outcomes: |
|
|
|
|
|
|
Has the applicant had any history of cruelty to animals? |
|
|
Yes |
No |
||
If yes, provide: Date(s): |
|
|
|
|
||
Outcomes: |
|
|
|
|
|
|
Has the applicant attempted suicide or had suicidal ideations? |
|
Yes |
No |
|||
If yes, provide: Date(s): |
|
|
|
|
||
Outcomes: |
|
|
|
|
|
|
Has the applicant had any history of fire setting? |
|
|
Yes |
No |
||
If yes, provide: Date(s): |
|
|
|
|
||
Outcomes: |
|
|
|
|
|
|
Has the applicant had any history of cutting self, swallowing or insertion of foreign objects or |
Yes |
No |
||||
strangulation? |
|
|
|
|
||
If yes, provide: Date(s): |
|
|
|
|
||
Outcomes: |
|
|
|
|
|
|
Has the applicant had physical aggression that required physical, mechanical or chemical restraint |
|
|
||||
via injection over the past 12 months? |
|
|
Yes |
No |
||
Page|2 of 5 |
Revised 03.17 |
FAMILY INFORMATION
Mother’s Name (first & last):
Address:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Telephone #: |
|
|
|
|
Work Telephone #: |
|
|
|
|
|||||||
Email Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Father’s Name (first & last): |
|
|
|
|
|
|
|
|
|
|
|
|||||
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Home Telephone #: |
|
|
|
|
Work Telephone #: |
|
|
|
|
|||||||
Email Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Sibling’s Full Name(s) (first & last): |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
Significant Other Name (first & last): |
|
|
|
|
|
|
|
|
||||||||
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Home Telephone #: |
|
|
|
|
Work Telephone #: |
|
|
|
|
|||||||
Email Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
APPLICANT’S FINANCIAL INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|||||
Receive Financial Assistance: |
|
|
|
Yes |
No |
|
|
|
|
|
|
|||||
If yes, type: |
SS (Social Security) |
SSI (Supplemental Social Insurance) |
|
|
|
|||||||||||
If other, document type: |
|
VA (Veteran’s Benefits) |
Child Support |
Adoption Subsidy |
Other |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
Does applicant have Title 19? |
|
|
|
Yes |
No |
|
|
|
|
|
|
|||||
Managed Care Organization (MCO)? |
Amerihealth Caritas |
Amerigroup |
United Health |
Optum N/A |
|
|
||||||||||
Does applicant have Waiver funding? |
Yes |
No |
|
|
|
|
|
|
||||||||
Does applicant have Habilitation funding? |
Yes |
No |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Does applicant have private insurance? |
Yes |
No |
|
|
|
|
|
|
||||||||
Does applicant have other income (trust fund, etc.)? |
Yes |
No |
|
|
|
|
||||||||||
APPLICANT’S HEALTH/MEDICAL INFORMATION
Current Medication(s) or can attach current medication orders or record:
Name |
|
Dose |
Frequency |
Reason for Taking |
|
|
|
|
|
|
|
|
|
|
Prescribed By
Page|3 of 5 |
Revised 03.17 |
Physical disabilities that require the use of adaptations (e.g. AFOs {braces}, orthopedic shoes, cane, walker, wheelchair,
etc.) |
Yes |
No |
|
|
|
|
|
|
If yes, list adaptive equipment: |
|
|
|
|
|
|||
Seizures: |
Yes |
No |
History of |
|
|
|
|
|
If yes or history of, describe type and frequency: |
|
|
||||||
Vision Problems: |
No |
Yes – correctable with glasses |
Yes – but chooses not to wear glasses |
|||||
|
|
Yes - uncorrected |
Blind Comments: |
|
|
|||
Hearing Problems: |
No |
Yes – correctable with hearing aides |
Yes – but chooses not to wear hearing aides |
|||||
|
|
Adapt by others speaking louder |
Deaf |
|||||
Comments:
Skill Checklist: (please check items which best describe applicant)
BEHAVIOR |
Consistently Sometimes Never Comments |
|
Becomes upset when |
|
|
redirected/corrected |
|
|
Demands excessive |
|
|
attention from others |
|
|
Complains of being |
|
|
persecuted |
|
|
Pretends to be ill |
|
|
Changes mood without reason |
|
|
Bosses or manipulates others |
|
|
Hyperactive |
|
|
Hoards things |
|
|
PICA (eats inedible objects) (if |
|
|
displays, list items in |
|
|
comments) |
|
|
Self stimulation |
|
|
Self injurious behavior |
|
|
Verbally aggressive |
|
|
Physically aggressive toward |
|
|
others |
|
|
Physcially aggressive toward |
|
|
objects |
|
|
Displays sexually inapprorpriate |
|
|
behavior |
|
|
Removes clothing in public |
|
|
Tears clothing |
|
|
Steals other's belongings |
|
|
Elopes / runs away from home |
|
|
Uses tobacco |
|
|
Uses alcohol |
|
|
Uses other drugs |
|
|
Page|4 of 5 |
Revised 03.17 |
LEISURE ACTIVITIES
Interests:
Hobbies:
Dislikes:
CLOSING
The information we have asked you to provide is necessary for the effective administration of the services for which you are applying. The information collected will only be used by authorized agency personnel. Use of this information for purposes other than expressed herein will not occur without your prior written approval, unless such other use is specifically authorized by law.
Attach any of the following materials that may be helpful in determining eligibility for service:
Most recent psychological evaluation
Most recent education and/or vocational report
Most recent progress reports or plan of care
Physical and/or specialty medical examinations
Other Documentation that you feel would be helpful
Completed by: |
|
||||
Applicant Name: |
|
Date: |
|||
Case Manager Name: |
|
Date: |
|||
Parent/Guardian Name: |
|
Date: |
|||
Name/Title: |
|
Date: |
|||
Please return form to: REM Iowa (please check website for current contact information @ www.remiowa.com)
or send to REMIowaReferral@thementornetwork.com
Page|5 of 5 |
Revised 03.17 |